Fracture Surgery
Plate and Screw Fixation
Fracture fixation using Plates and Screws
Intramedullary Nailing
Long rod used for Fracture fixations
Proximal Femoral Nailing
Rod fixation for Hip Fractures
K-wire fixation
Thin wire Fracture fixation
External Fixation
By Pins and rods outside the body


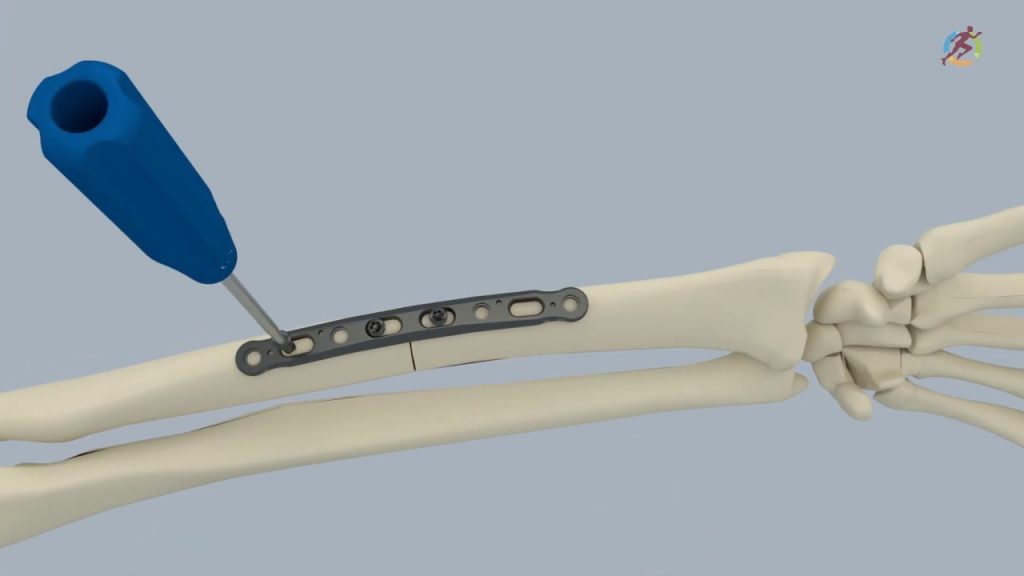

Plate and screw fixation of fracture is one of the most common orthopaedic intervention for fracture management. The procedure involves reducing the displaced fracture fragments and fixing it rigidly by a long linear metal implant (plate) to the bone. Screws are used to facilitate this fixation.
When is this surgery performed?
This is one of the most common and successful orthopaedic surgery, used when:
- The fracture is displaced
- Fracture cannot heal properly with immobilization alone
- Multiple fracture fragments
- Weight/stress bearing bone
- Intra-articular fracture
The surgery is performed by the concept of Open reduction internal fixation (ORIF). The steps involved in any plate fixation are as follows:
- The surgery is done by General, Spinal or regional anasthesis depending on the site of fracture and surgeons preference.
- An incision is made over the fractured bone (based on years of research done to reduce the number of muscle split and safely avoid any nerves and blood vessels)
- The fracture site is approached by retracting the overlying muscles and structures.
- The fracture is reduced with the help of special instruments and reduction is confirmed both visibly and by C-arm (xray machine).
- A plate of appropriate length is selected and placed over the bone and fixed on either end using multiple screws (number of screws deemed necessary by the surgeon).
- The reducion instruments are removed and the fracture stability is assessed by moving the joints above and below.
- Once the fixation is confirmed to be stable the wound is closed and dressing applied.
- Sometimes a plaster slab may be applied in certain fractures to reduce post-operative edema, added stability and faster recovery.
Lifting heavy weights is avoided for few days in upperlimb fracture fixation. Weight-bearing is avoided for few days in lower limb fracture fixation.
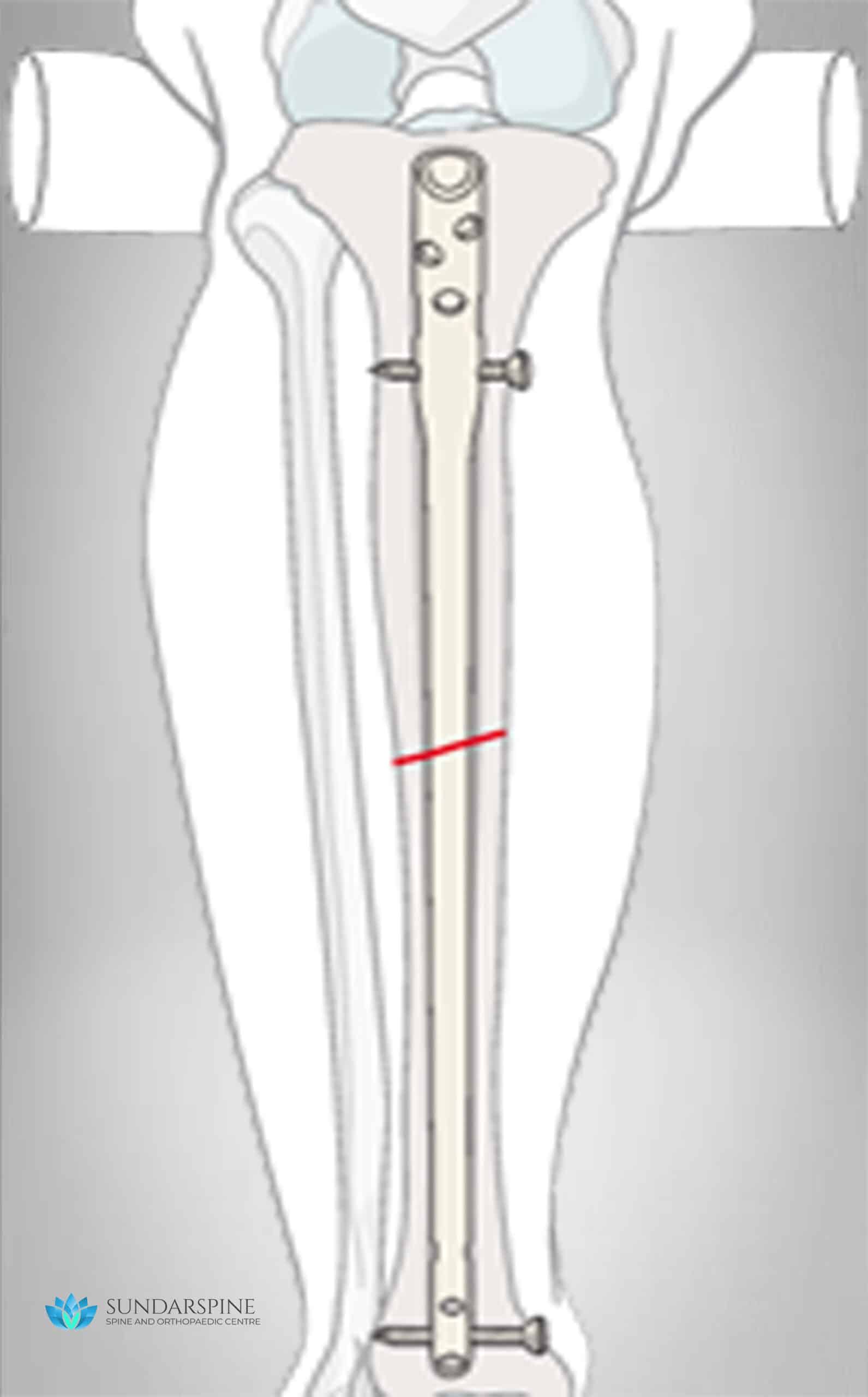

Intramedullary nailing (IM Nailing) is a technique of fracture fixation commonly used in long bones – thigh bone (femur), Leg bone (tibia) and the arm bone (humerus). This technique has is mainly prefered for weight-bearing bones as they give more stability and support early walking after surgery.
When is this surgery performed?
This technique can be done only in very specific type of fractures:
- Shaft (middle) and proximal fracture of the thigh bone (femur)
- Shaft (middle) fracture of the leg bone (tibia)
- Shaft (middle) fracture of the arm bone (humerus)
Advantages of this procedure:
- Early weight bearing
- Smaller incision (compared to plating)
- Incision not over the fracture site – faster healing
- Lesser blood loss
- More stable
- Faster bone union
The surgery is performed by the concept of Closed reduction and internal fixation (CRIF). The steps involved in any intramedullary nailing are as follows:
- The surgery is done by Spinal anasthesia (lower limb) and general or regional anasthesia (upper limb).
- An incision is made over one end of the bone near the joint.
- The bone is entered with a sharp instrument and the hollow middle (medullary cavity) of the bone is approached.
- A guide wire is inserted through the hole which is passed to the full length of the bone crossing the fracture site.
- Certain manipulation is required to pass the guide wire across the fracture site. (confirmed by C-arm)
- The medullary cavity is reamed (widened) to accomodate the implant – nail.
- The implant – Intramedullary Nail is introduced through this canal and fixed by screws both far above and below the fracture site.
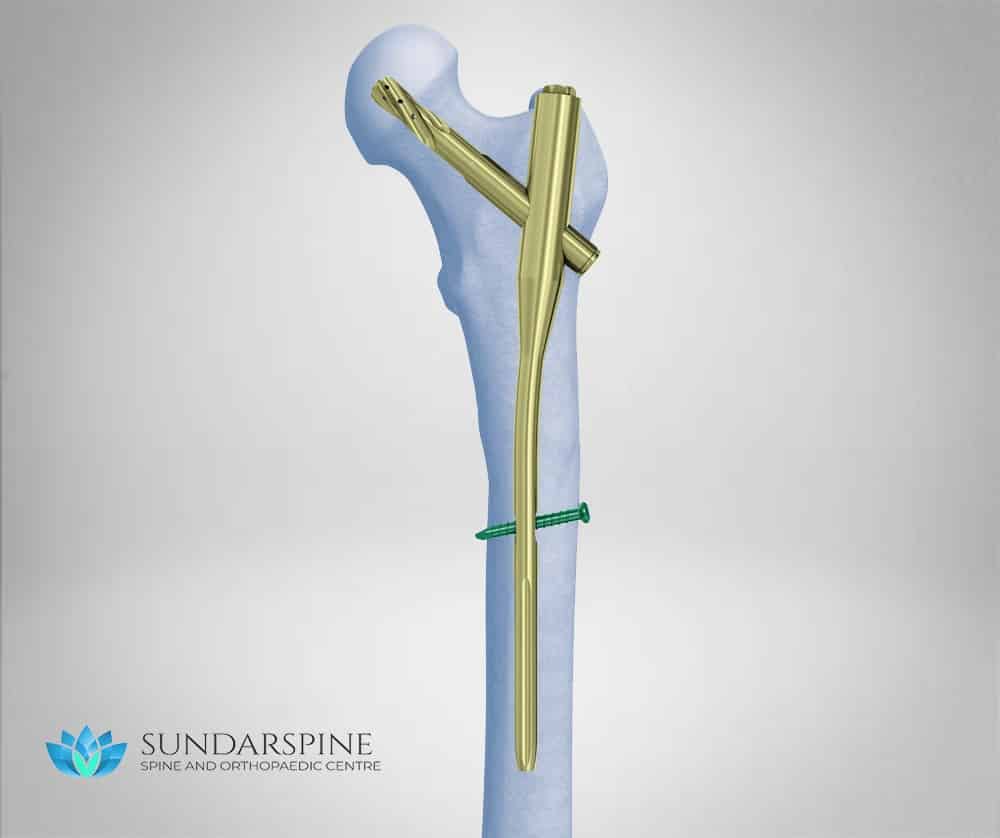

Proximal Femoral nailing is a technique of fracture fixation that is used to treat hip fractures (Proximal femur). Hip fractures are the most common type of fracture especially in the elderly.
When is this surgery performed?
This technique can be done only in very specific type of fractures:
- Hip fracture (intertrochanteric)
- Upper thigh fracture (Subtrochanteric)
Advantages of this procedure:
- Early weight bearing
- Smaller incision (compared to plating)
- Incision not over the fracture site – faster healing
- Lesser blood loss
- More stable
- Faster bone union
The surgery is performed by the concept of Closed reduction and internal fixation (CRIF). The steps involved are as follows:
- The surgery is generally done by Spinal anasthesia.
- The fracture is reduced by manipulation on a fracture table before incision.
- An 8-10cm incision is made over the uppermost end of the thigh where the thigh bone (femur) starts.
- The bone is entered with a sharp instrument and the hollow middle (medullary cavity) of the bone is approached.
- A guide wire is inserted through the hole which is passed to the full length of the bone crossing the fracture site.
- The medullary cavity is reamed (widened) to accomodate the implant – proximal femoral nail.
- The implant may be a short nail (intertrochanteric fracture) or a long nail (subtrochanteric fracture).
- The nail is fixed by using a special blade/screw in the upper side and normal screw on the lower side though seperate small incisions.
Brace : Nil
K-wire fixation
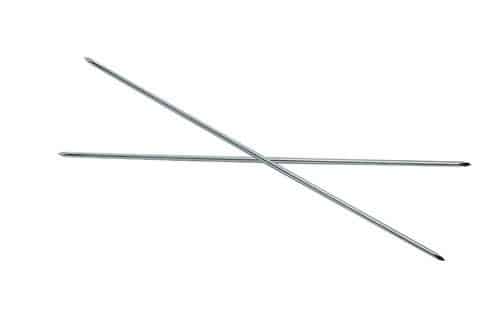
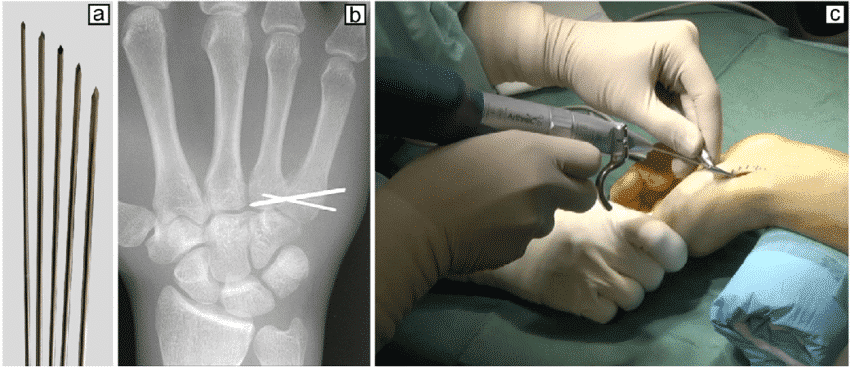


K-wire is a thin metallic pin/wire like structure that is used to fix or stabilize a fracture. They are normally used to fix fractures of the small bones (hands or foot) or larger bones in children. They do not have inherent stability, hence are usually used along with splints or braces till fracture stability.
How the surgery is performed?
- The procedure is usually performed under light sedation or regional block depending on the age and location of fracture.
- The fracture is reduced by manipulation under C-arm
- The k-wire of appropriate diameter is introduced with the help of a drill.
- The wire is usually engaged into the opposite bone across the fracture holding both the fragments in reduced position.
- Usually more than one k-wire might be required to fix fragments in both planes.
- The other end of k-wire is usually left outside or can be buried inside the skin with sutures.
- The procedure is usually supplemented by a splint or a brace.
The k-wire necessitates removal after 3-6 weeks. The exposed k-wire can be removed in outpatient procedure room whereas the buried k-wire require local/regional anasthesia and hence might be done as an operative room procedure.
Advantages of K-wire:
Holds the fracture fragments in reduced position till the fracture heals. Multiple k-wires increase the stability of the fracture fixation.
Recovery time:
Duration of surgery: 1-2 hours
Walking started: Variable
Hospital stay: 1-2 days
Resume work: After k-wire removal
Brace (Splints): 3-6 weeks
Driving (Car, Bike): After k-wire removal
Strenuous Activity (bending down, lifting weights): Variable
External Fixator


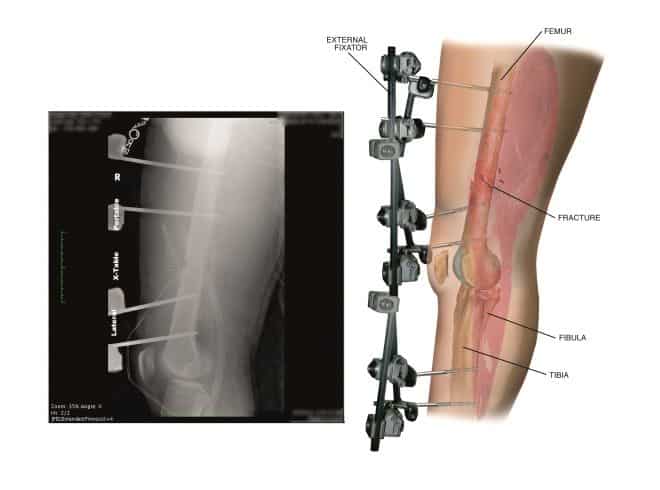

- External Fixator is a technique of holding the fracture fragments by a pin connected to a rod externally, until the skin and soft tissue heals.
This procedure is usually done in open fracture or in severe multiple injuries to give adequate time for healing before the main final fixation.
When is this Surgery performed?
- In severe open fracture
- Multiple long bone or pelvic fracture
- Complex fracture near joints (knee, wrist or ankle)
- Fracture with associated life threatening injuries.
- As a temporary stabilization till the patient is fit for the main procedure.
- The surgery can be performed under general, regional or spinal anasthesia.
- The fracture is reduced under C-arm guidance and multiple pins are placed above and below the fracture site.
- All the pins are connected by a rod which holds the fracture in relative stability.
Advantages of External fixator:
This procedure is usually done as a temporary stabilization till the would and the patient are stable for further procedure. The initial 3 days after a high velocity is a risk period for both the wound (increased swelling, infection) and the patient (risk to life). Hence major procedure such as final fixation are avoided during this period.
Using Restroom: Variable
Spine Surgery
Surgeries of the Neck and Back
Micro-Discectomy
Removal of the Disc
Interbody Fusion
Fusing abnormal Vertebra
ACDF
Disc Surgery of the Neck
Neck Corpectomy
Vertebral Surgery of the Neck
Thorasic Corpectomy (Back)
Vertebral Surgery of the Back
Vertebroplasty
Cement Injection for Fractures
Kyphoplasty
Balloon inflation of Collapsed vertebra
Scoliosis Surgery
Scoliosis Deformity Correction
Endoscopic Surgery
Pen-hole, Key-hole Surgery
Fracture Surgery
Surgical Management of all Fractures
Plate and Screw Fixation
Fracture fixation using Plates and Screws
Intramedullary Nailing
Long rod used for Fracture fixations
Proximal Femoral Nailing
Rod fixation for Hip Fractures
K-wire fixation
Thin wire Fracture fixation
External Fixation
By Pins and rods outside the body
Joint Replacements
Arthroplasty
Hip replacement
Hemiarthroplasty, Total Hip Replacement
Knee replacement
Unicondylar and Total Knee Replacement
Shoulder replacement
Hemi, Total and Reverse Shoulder Arthroplasty

Our World, Our Vision
We at SUNDARSPINE, believe in our promise to the world to provide Free access Healthcare Education to everyone. This site is a result of years of Planning and Hardwork. We are dedicated to help in your patient experience and aspire to increase our network globally and include a complete database of all health related information and guidance. We have just begun and we have a long way to go. Thank you in being a part of Us!!
We’d love to hear from you
Have any questions, Checkout
Download a FREE Ebook
Subscribe to our news letter